Newcastle University Press Office Published on: 5 December 2017
Almost half of the patients with Type 2 diabetes supported by their GPs on a weight loss programme were able to reverse their diabetes in a year, a study has found.
Professor Roy Taylor
The first year results, which are published today in TheLancet, also revealed that almost nine out of 10 people (86%) who lost 15kg or more put their Type 2 diabetes into remission.
The study led by Professor Roy Taylor, from Newcastle University, and Professor Mike lean from Glasgow University, found that 45.6% of those who were put on a low calorie diet for three to five months and were able to stop their Type 2 diabetes medications.
Importantly, long-term support by routine General Practice staff was given to help the paticipants maintain their weight loss.
The trial, called DiRECT (Diabetes Remission Clinical Trial) and funded by Diabetes UK, recruited 298 people between the Newcastle and Glasgow University and builds on Professor Taylor’s earlier pilot work.
Professor Taylor, lead researcher of the DiRECT trial, said: “These findings are very exciting. They could revolutionise the way Type 2 diabetes is treated.
“The study builds on the work into the underlying cause of the condition, so that we can target management effectively.
“Substantial weight loss results in reduced fat inside the liver and pancreas, allowing these organs to return to normal function.
“What we’re seeing from DiRECT is that losing weight isn’t just linked to better management of Type 2 diabetes: significant weight loss could actually result in lasting remission."
Remission achieved
Remission was defined as having blood glucose levels (HbA1c) of less than 6.5% (48mmol/mol) at 12 months, with at least two months without any Type 2 diabetes medications.
Of the 298 people recruited to take part in DiRECT, half received standard diabetes care from their GP, whilst the other half received a structured weight management programme within primary care.
The programme included a low calorie, nutrient-complete diet for three to five months, food reintroduction and long-term support to maintain weight loss.
Type 2 diabetes remission was found to be closely related to weight loss. Over half (57%) of those who lost 10 to 15kg achieved remission, along with a third (34%) of those who lost five to 10kg. Only 4% of the control group achieved remission.
The findings have been presented at the International Diabetes Federation Congress in Abu Dhabi today by the lead researchers, Professor Taylor and Professor Mike Lean.
Professor Lean said: “Putting Type 2 diabetes into remission as early as possible after diagnosis could have extraordinary benefits, both for the individual and the NHS. DiRECT is telling us it could be possible for as many as half of patients to achieve this in routine primary care, and without drugs.
“We’ve found that people were really interested in this approach – almost a third of those who were asked to take part in the study agreed. This is much higher than usual acceptance rates for diabetes clinical trials."
Two-year trial
DiRECT is a two-year trial which aims to find an effective and accessible way to put Type 2 diabetes into remission for the long-term.
The trial is delivered through GP practices across Tyneside and Scotland to find out if the benefits of a structured weight management programme can be felt in a real-life primary care setting.
DiRECT also aims to understand why significant weight loss results in remission, to understand which groups might benefit in the future.
Type 2 diabetes is a life-changing condition that progresses over time, which can have devastating consequences. Finding ways to put it into lasting remission could significantly reduce the cost of delivering diabetes care and treating serious complications such as cardiovascular disease, kidney disease or stroke.
Remission could transform the lives of millions of people living with or at risk of Type 2 diabetes.
Isobel Murray, 65, from North Ayrshire, took part in DiRECT from 2014 to 2016. She was on the low calorie diet programme for 17 weeks and put her Type 2 diabetes into remission after the first four months.
Over the two year trial, Isobel lost more than three and a half stone and no longer needs to take any diabetes medication.
Isobel said: “It has transformed my life, I had Type 2 diabetes for two to three years before the study.
“I was on various medications which were constantly increasing and I was becoming more and more ill every day. When the opportunity came to go on the DiRECT study, I had absolutely no hesitation.
“When the doctors told me that my pancreas was working again, it felt fantastic, absolutely amazing.
“I don’t think of myself as a diabetic anymore, I get all my diabetes checks done, but I don’t feel like a diabetic. I am one of the lucky ones to have gone into remission.”
Diabetes UK has committed more than £2.8 million to the DiRECT study. Recently, £300,000 has been committed so participants who wish to continue can be followed for up to three years and the full cost-effectiveness of this programme can be evaluated.
The funding will provide further understanding around the longer term benefits, to see if a treatment of this kind could be offered to people with Type 2 diabetes in the future.
Helping millions
Dr Elizabeth Robertson, Director of Research at Diabetes UK, said: “These first year findings of DiRECT demonstrate the potential to transform the lives of millions of people.
“We’re very encouraged by these initial results, and the building robust evidence that remission could be achievable for some people.
“The trial is ongoing, so that we can understand the long-term effects of an approach like this. It’s very important that anyone living with Type 2 diabetes considering losing weight in this way seeks support and advice from a healthcare professional.”
Whether putting Type 2 diabetes into remission can protect against diabetes-related complications later in life is not yet known, which is why it is important that those who achieve remission continue to receive health checks.
More research is also needed to find out who could benefit most from treatments like this in the future, taking into account factors like ethnicity and duration of Type 2 diabetes.
The Prospective Urban Rural Epidemiology (PURE) study is a large, epidemiological cohort study of individuals aged 35–70 years (enrolled between Jan 1, 2003, and March 31, 2013) in 18 countries with a median follow-up of 7·4 years (IQR 5·3–9·3). Dietary intake of 135 335 individuals was recorded using validated food frequency questionnaires. The primary outcomes were total mortality and major cardiovascular events (fatal cardiovascular disease, non-fatal myocardial infarction, stroke, and heart failure). Secondary outcomes were all myocardial infarctions, stroke, cardiovascular disease mortality, and non-cardiovascular disease mortality. Participants were categorised into quintiles of nutrient intake (carbohydrate, fats, and protein) based on percentage of energy provided by nutrients. We assessed the associations between consumption of carbohydrate, total fat, and each type of fat with cardiovascular disease and total mortality. We calculated hazard ratios (HRs) using a multivariable Cox frailty model with random intercepts to account for centre clustering
Carbohydrates, Fats, and CVD in the PURE Study
Carbohydrate intake was divided into quintiles. Those in Q5 consumed most, and those in Q1 consumed least. As can be seen from the slide below, presented by Dr. Yusuf, using the lowest carbohydrate intake (Q1) as a reference, there is an increased risk of CVD with increasing carbohydrate consumption.
Dr. Yusuf pointed out that earlier dietary guidelines “said reduce fats and compensate for it by carbohydrates. So essentially we’ve increased carbohydrate intake in most Western countries, and this is likely damaging.”
Furthermore, Yusuf said:“We were in for a big surprise. We actually found that increasing fats was protective. Now, these are all fats. So this very first slide challenges the WHO and the AHA guidelines on diet.”
With regards to carbohydrates as a percentage of daily energy consumption, he also said: “once you get past about 40% or about 55% of carbohydrate intake as percent energy, there is a steep increase in the risk of CVD. The WHO guidelines say that up to about 75% of carbohydrates is ok. But that is wrong.”
Then he adds:
“Again, total fats, if anything, is protective. And the reasons for this are twofold. Too low fat is inadequate, too high fat is probably bad. And the original studies from Finland was at extremely high fat levels, not the usual fat levels that populations consume.
Does the Type of Fat Matter?
Current dietary guidelines recommend that we limit the intake of saturated fats and replace them by mono- and polyunsaturated fats. Low-fat dairy products are recommended for the purpose of avoiding saturated fats. Vegetable oils should be used instead of butter.
As Dr. Yusuf points out, these recommendations are not supported by data from the PURE study:
“Then if you look at the types of fats, saturated fats, you will see there is not really a clear pattern of anything. Within the normal range, saturated fats are not harmful. May even be slightly beneficial. But there is no harm.
With monounsaturated fatty acids which are in olive oil, canola oil, and are part of the key to the Mediterranean diet, you get a clear benefit. Polyunsaturated fatty acids which are largely from vegetable oils, and remember that is processed oil, is largely neutral.
So, fundamentally, our fat story is: some fats are good, some fats may be neutral but it is carbohydrates that are the worst thing.”
“The other thing is; in the US there is this big swing to reduce milk consumption, and even if you consume milk, they want you to consume 2% or 1% of fat. What is the evidence? A big zero. Absolutely no evidence that low-fat milk is better for you. If anything, if you look at dairy sources of saturated fats, it is protective.
If you look at meat sources of fat, saturated fats, it’s neutral. And if you look at white meat such as chicken and fish, there is a trend towards benefit. So, red meat in moderate quantities is not bad and white meat may be moderately beneficial. But dairy fats such as cheese are probably good for you, and milk, there is really no data at all to reduce the fat content of milk.”
Saturated Fats, LDL-Cholesterol, and CVD
Dr. Yusuf says:
“Now, why did we go wrong. We went wrong because of surrogate end-points.
The story on saturated fats vs. LDL is consistent. Our data shows that as you increase the amount of saturated fats, your LDL goes up. But first, look at how much LDL goes up. This is a 150 thousand people in the analysis – from about 2.85 (108 mg/dL) to just under 3 (116 mg/dL). About 0.1 mmol/L (3.9 mg/dL) increase over a huge range of percentage of saturated fat (consumption).
But CVD shows exactly the opposite end-point.
Macronutrients and the ApoA/ApoB Ratio
Dr. Yusuf also addresses the effects of carbohydrate intake on more advanced lipoprotein measurements:
“Now, what about carbohydrate intake? If you look at LDL, there will be an inverse relationship. But if you look at ApoB/ApoA ratio, which today we know is the most sensitive marker for risk prediction there is a steep increase – from about 0.72 to nearly 0.85 with increasing carbohydrate intake. But with saturated fats, if anything, it is neutral or tending to go down.”
Final Remarks
Dr. Yusuf’s final remarks include these words:
“Contrary to common beliefs, the current recommendations to reduce saturated fats have no scientific basis. I’m not the only one saying this. You must have heard of the book called ‘The Big Fat Surprise’ by Nina Teicholz. She shook up the nutrition world, but she got it right.
Did you know that the seven countries studies that actually had a straight line between fat intake and CVD is fudged. I’m using the word fudged because 23 countries participated in that study and they took the seven best that fitted that line, and that’s what’s there. If you go through the literature, you will find that they chose the seven that fitted the line. The nutrition field has been distorted.”
So, is there a time for a reappraisal of public recommendations regarding the relationship between diet and heart disease following the presentation of the PURE date on macronutrients.
Obviously, this is a rhetorical question. Let’s get to work.
Hand out di bawah ini saya berikan kepada pesakit-pesakit yang mempunyai diabetis atau yang ingin mengurangkan berat badan..alhamdulillah ramai yang telah berjaya menurunkan paras gula, menurunkan berat badan serta tekanan darah..
(Dengan pengawasan doktor bertauliah,
terutama jika anda sedang mengambil ubat/insulin untuk diabetis)
1 1)Puasa berkala (intermittent fasting)
a)Formula 16:8 iaitu
puasa selama 16 jam dan sela masa makan selama 8 jam
Cth: last makan malam pukul 8.00 malam dan keesokan harinya
anda ‘skip’ breakfast dan makan tengahari pukul 12.00 tengahari.
Maksudnya ‘puasa separuh hari’ dan
anda hanya makan 2 kali sehari (lunch, dinner)
Dibolehkan minum air
kosong @ kopi @ the tanpa gula(blh dicampur stevia jika perlu) semasa tempoh
puasa. Tidak digalakkan ‘snacking’
b)Puasa penuh 2x seminggu (cth isnin
& khamis)
c)Puasa penuh selang sehari
Nota: Tujuan
puasa adalah supaya tubuh membakar simpanan gula (glikogen) dan seterusnya
lemak yang tersimpan dalam tubuh akan dibakar sebagai
sumber tenaga . Proses ini akan berterusan selagi anda tidak mengambil minuman
@ makanan manis/berkarbohidrat tinggi
2 2)Diet Rendah Karbo & Lemak Sihat (RKLS)
Apa yang boleh dimakan?
Contoh diet RKLS
Contoh diet RKLS
Asasnya makanan yang mengandungi karbo rendah, kandungan protein
sederhana tinggi serta lemak yang sihat.Ambillah makanan yang semulajadi, segar
dan bukan yang diproses @ makanan segera. Elakkan MSG (terutama makan di luar)
kerana MSG boleh meningkatkan paras insulin
·Karbo: < 50 gm sehari. Kurangkan
pengambilan karbo berkanji (ingat: ianya hanya rantaian gula!) seperti nasi,
roti dan pasta. Gula makan- elakkan sama sekali!
Biskut dan kek-adalah
kombinasi gula dan karbo yang perlu dielakkan sama sekali kerana ia menyebabkan
anda lebih ketagih kepada gula dan menyebabkan anda lebih cepat lapar!
Contoh karbo 50 gm
Semua sayuran hijau/salad
adalah ok. Makan seberapa banyak yang anda mahu.Biar anda kenyang dengan
sayur/ulam dan lauk.Jika ingin juga mengambil nasi, pastikan sangat minimum
(kira-kira ¼ pinggan). Digalakkan mencuba beras perang atau barli menggantikan beras putih
biasa. Tip: Bagi yang bekerja, boleh mencuba sup yang dimasak di rumah dan
dibawa ke tempat kerja. Lebihkan cendawan, tomato dan bawang di dalam sup.
Buah-buahan?
Buah-buahan hanya dimakan
secara‘raw’ dan tidak dibuat
jus.Buah-buahan yang boleh dimakan adalah seperti strawberi, epal dan pear
tetapi buah-buahan tempatan seperti pisang, tembikai, mangga dan nenas TIDAK
digalakkan kerana mengandungi gula yang tinggi
·Protein – contoh ikan, ayam, daging dan
telur perlu diambil dengan agak banyak. Panduan: sekitar 4 saiz tapak tangan
sehari( wanitasekitar 80 gm, lelaki sekitar 120
gm sehari). Daging yang diproses seperti dalam burger, nuggets atau
sosej adalah tidak berapa menyihatkan dan perlu diambil sekali sekala sahaja
·Lemak (Jangan takut kepada lemak!) perlu
diambil dalam kuantiti yang sederhana (dilebihkan). Lemak yang baik adalah
seperti yang terdapat dalam minyak kelapa, minyak sawit atau minyak zaitun.
Minyak kelapa adalah yang terbaik untuk menggoreng kerana ia paling stabil.
Gantikan marjerin dengan mentega yang lebih menyihatkan. Juga boleh mengambil
yoghurt tinggi lemak. Vitamin A, D, E dan K hanya boleh didapati dalam
makanan berlemak dan berminyak. Elakkan
marjerin, minyak jagung dan minyak sayuran. Hati-hati makanan ‘rendah lemak’ kerana biasanya ia mengandungi gula yang tinggi atau pemanis tiruan! #SukuSukuSeparuh . (Jika anda rasa diet di atas sangat extreme) Ini portion mudah untuk diikuti seperti yang disarankan Kementerian Kesihatan Malaysia: -Suku pinggan: lauk (protein, lemak) -Suku pinggan : karbo (nasi) -Separuh pinggan : sayur-sayuran/ulam
MAKAN BANYAK SAYURAN DENGAN PROTEIN
DAN LEMAK YANG BAIK MENYEBABKAN ANDA LAMBAT LAPAR DAN INI MENSTABILKAN PARAS GULA DAN ANDA AKAN MEMBAKAR LEBIH BANYAK LEMAK
Disediakan oleh:
~Dr Hapizi
WA:
0179351516
Email :
dr_hapizi@yahoo.com
p/s: Selepas mencuba, sila hantar feedback anda kepada saya ya! (Melalui whatsap atau email)
-artikel ini dibenarkan utk dikongsi, tanpa kebenaran saya.
Oleh: Dr Ahmad Hapizi Abdullah
(Artikel ini dihantar untuk diterbitkan oleh sebuah akhbar online)
“Wahai orang-orang yang
beriman, diwajibkan atas kamu untuk berpuasa sebagaimana diwajibkan atas
orang-orang sebelum kamu agar kamu bertaqwa..” (Surah Al-Baqarah:183)
Ayat di atas
selalu kita dengar setiap kali menjelangnya bulan Ramadan al mubarak yang kita
sama-sama akan menyambutnya tidak berapa lama lagi
Allah SWT
sebagai Pencipta manusia pastilah Maha Mengetahui hikmah diwajibkan berpuasa
selama sebulan penuh setiap tahun kepada setiap orang Islam kecuali jika
mempunyai keuzuran tertentu.
Antara manfaat
berpuasa secara umum adalah dari aspek kerohanian (meningkatkan keimanan,
menjadi insan lebih bertaqwa, melatih kesabaran, mengawal hawa nafsu dan
sebagainya), aspek psikologi (melatih
kemampuan mengawal diri, disiplin, mengurus masa, wang dan sebagainya) serta
aspek fizikal iaitu kesihatan.
Artikel ini akan memfokus kepada manfaat berpuasa dari aspek
kesihatan.
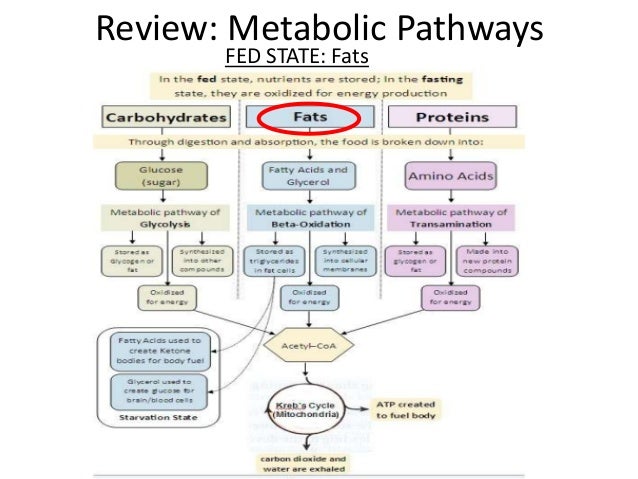
Sebelum itu ada baiknya kita memahami secara ringkas, proses
fisiologi normal yang berlaku apabila kita makan (fed state) dan apabila kita berpuasa (fasted state). Kedua-dua keadaan ini saling berkaitan tetapi
berlawanan antara satu sama lain (ibarat ‘yin’ dan ‘yang’)
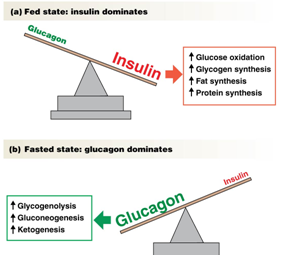
Sebaik sahaja kita makan, hormon insulin akan dirembeskan
sebanyak-banyaknya dan insulin akan memberi isyarat kepada tubuh untuk
menyimpan kalori sebagai lemak. Insulin juga akan menghalang pembakaran lemak
Dalam keadaan kita berpuasa, paras insulin adalah rendah
(manakala hormon glukagon dan hormon pertumbuhan (growth hormone) yang mempunyai fungsi berlawanan dengan insulin,
meningkat naik.
Secara ringkasnya insulin boleh diibaratkan sebagai “suis”
yang mengawal samada lemak disimpan atau dibakar
Apakah kepentingan anda mengetahui asas ini? Anda hanya boleh
membakar lemak dalam keadaan berpuasa dan anda hanya boleh menambah lebih
banyak lemak semasa anda kekenyangan!
Kerintangan Insulin
Akibat dari tabiat makan yang berlebihan di negara ini, kita
berada dalam keadaan kekenyangan (fed
state) dalam kebanyakan masa, cuma waktu tidur sahaja kita berada dalam
keadaan puasa (fasted state).
Kesannya sel-sel badan kita sentiasa ‘dibanjiri’ hormon insulin yang tinggi dan
kurang membakar lemak, sebaliknya pula lemak semakin lama semakin banyak
tersimpan dalam tubuh.
Akhirnya paras insulin yang tinggi sepanjang masa menyebabkan
tubuh kita hanya bergantung kepada glukosa sebagai sumber tenaga dan pendedahan
kepada insulin lama kelamaan menyebabkan sel-sel tubuh menjadi rintang (“immuned”) kepada insulin dan lebih
banyak hormon tersebut dirembeskan, menjadi suatu pusingan yang tak
berkesudahan (vicious cycle).
Kerintangan insulin yang kronik adalah punca kepada sindrom
metabolik yang ditandai dengan obesiti, pengumpulan lemak bahagian abdomen,
paras trigliserida tinggi, rendah HDL (‘kolesterol baik’) dan akhirnya boleh
membawa kepada diabetis.
Adaptasi lemak
Tubuh manusia mempunyai kebolehan untuk membakar lemak,
bukannya glukosa sebagai sumber tenaga. Ini tentunya perlu kepada masa dan
latihan tertentu, terutama dari pengubahsuaian dari segi pengambilan makanan
yang betul
Ada beberapa cara untuk mencapai keadaan diatas, antaranya
pengambilan diet rendah karbohidrat, bersenam, pengambilan makanan kalori
rendah dan berpuasa secara berkala (intermittent
fasting)
Puasa berkala (intermittent fasting)
Menurut Dr. Jason Fung, seorang Pakar Perubatan buah pinggang
dari Kanada dan antara peneraju dan penyelidik dalam bidang ini menegaskan,
antara manfaat puasa berkala adalah merangsang pembakaran lemak, meningkatkan
kesensitifan terhadap insulin, meningkatkan metabolisma, meningkatkan fungsi
otak, mengaktifkan sistem pertahanan badan, membaiki masalah hati berlemak,
merencat sel-sel kanser, mengurangkan proses inflamasi, merendahkan tekanan
darah, menurunkan kadar kolesterol dan banyak lagi.
Formula 16:8
Antara kaedah yang
disarankan oleh Dr Jason Fung ialah formula 16:8, iaitu anda berpuasa selama 16
jam dan makan hanya dalam selang masa 8 jam berikutnya. Contohnya makan malam
yang terakhir anda adalah pada jam 8.00 malam. Selepas itu anda jangan makan
apa-apa kemudian masuk tidur. Keesokan paginya, anda jangan mengambil sarapan,
sebaliknya teruskan berpuasa sehingga jam 12.00 tengahari untuk makan
tengahari. Dari pukul 12.00 tengahari, anda boleh makan seperti biasa hingga
pukul 8.00 malam
Ini kerana tubuh kita
memerlukan masa sekurang-kurangnya 12 jam untuk memasuki fasa pembakaran lemak.
Berpuasa merangsang autofagi
Autofagi adalah
proses pembersihan terhadap komponen-komponen sel dan molekul yang rosak.
Pengumpulan bahan-bahan buangan sel ini akan menjadi toksik dan merosakkan
fungsi sel. Semasa keadaan kekenyangan dimana paras insulin adalah tinggi,
kadar proses autofagi ini adalah sangat rendah dan semasa berpuasa, kadarnya
meningkat sehingga 5 kali ganda!
Autofagi adalah
proses yang aktif semasa umur muda. Semakin umur meningkat, proses autofagi
semakin menurun dan menyebabkan kerosakan sel semakin bertambah, ditambah lagi
jika seseorang mempunyai diabetis.
Dengan mengamalkan
puasa berkala, didapati kadar autofagi menjadi aktif seperti pada usia muda!
Berpuasa sebagai terapi anti-penuaan
Kajian saintifik juga
mendapati puasa secara berkala memanjangkan telomere
iaitu struktur yang terdapat di hujung kromosom yang melindungi kromosom dari
kerosakan. Secara asasnya semakin panjang telomere
seseorang, didapati umurnya semakin panjang serta kesihatan seseorang secara
umumnya baik.
Paras saintis barat
sedang giat menyelidik dan mencipta ubat-ubatan serta terapi yang mahal untuk
memanjangkan telomere, jadi kenapa perlu ubat-ubat yang mahal, sedangkan anda
boleh melakukannya dengan mudah dan percuma? Berpuasa!
Puasa Ramadan
Jelaslah berpuasa di
bulan Ramadan adalah salah satu kaedah puasa berkala. Katalah kita bersahur
pada pukul 5.00 pagi dan berbuka pada pukul 7.20 malam. Itu sudah 14 jam lebih
berpuasa!
Selepas masuknya azan
subuh, kita akan mula berpuasa sehinggalah ke azan maghrib. Pada masa itulah
sel-sel tubuh kita akan menggunakan glukosa yang diambil semasa sahur, dan
apabila ini kehabisan, glikogen iaitu (simpanan glukosa yang berada dalam otot
dan hati akan dibakar). Apabila bekalan glikogen pula habis, tubuh akan
membakar lemak pula sebagai sumber tenaga.
Kajian-Kajian Saintifik Berkenaan Puasa Ramadan
Terdapat banyak
kajian yang telah dibuat berkenaan puasa Ramadan. Pada tahun 1996, sebuah
konferen antarabangsa telah berlangsung di Casablanca, Morocco dan sebanyak 50
kertas kajian dibentangkan. Kesimpulan dari konferen tersebut telah menunjukkan
puasa Ramadan mempunyai kesan positif terhadap kesihatan termasuk mengawal
kadar glukosa darah, menurunkan tekanan darah, membaiki profil kolesterol dan
kesan menurunkan berat badan. Tiada kesan sampingan serius dilaporkan.
Nasihat umum semasa Ramadan
Semasa berbuka dan
malamnya, kurangkan pengambilan minuman dan makanan manis serta berkarbohidrat
tinggi seperti air yang sangat manis, kuih muih yang manis dan nasi yang
berlebihan. Sebaliknya lebihkan pengambilan air kosong, makanan tinggi
kandungan serat (sayur-sayuran, buah-buahan) serta makanan yang yang mempunyai
kandungan protein dan lemak yang lebih tinggi.
Ini kerana minuman
atau makanan yang manis akan meninggikan kandungan insulin seterusnya merencat
proses pembakaran lemak. Apa yang kita mahu adalah tubuh terus menggunakan ‘mode’ pembakaran lemak, walaupun pada
malam-malam Ramadan!
Jadi makanlah secara
bersederhana, kalau ingin ‘bersenam’ pula, jangan lupa untuk bertarawih pada
malamnya. Dapat pahala dan kesihatan yang baik…insya Allah !
Dan apabila
berakhirnya Ramadan, ada baiknya kita meneruskan puasa berkala ini (puasa sunat
isnin dan khamis misalnya) serta mengurangkan pengambilan gula serta makanan
berkarbohidrat tinggi!
Excellent scientific explanation on aetiology of obesity by Dr Jason Fung, a Physician/Nephrologist from Canada.
Also detailed..the medical benefit of intermittent fasting as effective, safe, simple and doable method to combat obesity
(Donald Miller is a cardiac surgeon and Professor of Surgery at the University of Washington School of Medicine in Seattle)
Types and Structure of Fats
Crisco
Evidence Supporting the Lipid Hypothesis
Rabbits, Cholesterol, and Atherosclerosis
In 1913 a Russian physiologist fed high doses of cholesterol to rabbits and showed that cholesterol caused atherosclerotic changes in the rabbit’s arterial intima like that seen with human atherosclerosis. Over the ensuing decades other investigators did atherosclerosis research on cholesterol-fed rabbits, which they cited in support of the diet-cholesterol theory of heart disease.
Framingham Heart Study
In 1948, government-funded investigators began following some 5,000 men and women in Framingham, Massachusetts to see who developed coronary heart disease. They found that people with elevated cholesterol were more likely to be diagnosed with CHD and die from it.
Six years later the American Heart Association began promoting what it called the Prudent Diet, where "corn oil, margarine, chicken, and cold cereal replaced butter, lard, beef, and eggs."
Ancel Keys Six-Country and Seven-Country Studies
Ancel Keys, the father of K-rations for the military, published a study in 1953 that correlated deaths from heart disease with the percentage of calories from fat in the diet. He found that fat consumption was associated with an increased rate of death from heart disease in the six countries that he studied.
McGovern Report
The U.S. Senate Select Committee on Nutrition and Human Needs, chaired by Senator George McGovern, released, in 1977, its "Dietary Goals for the United States," designed to reduce fat intake and avoid cholesterol-rich foods. These dietary goals became become official government policy.
Further Developments
McDonalds and the Center for Science in the Public Interest
Next, in 1984 the Center for Science in the Public Interest, a consumer advocacy group, joined the fray and started to coerce fast-food restaurants and the food industry to stop baking and frying food with animal fats and tropical oils. McDonalds fried its French fries with beef fat and palm oil. That's why they tasted so good. But the Center for Science in the Public Interest’s well-orchestrated saturated fat attack coerced McDonalds and other fast-food chains to switch to partially hydrogenated, trans-fat vegetable oil.
USDA Food Pyramid
Dietary Guidelines for Americans 2010
Beginning in 1980, the U.S. Department of Agriculture and Department of Health and Human Services has published every five years an updated Dietary Guidelines for Americans. The most recent one, published in December 2010, recommends reducing saturated fat intake to 7 percent of caloric intake, down from its previously recommended 10 percent.
Meet the Fats
Other Countries with CHD-Death and Fat Consumption Data
Evidence against fat wilts upon close scrutiny. In his Six Country Study, Ancel Keys ignored data available from 16 other countries that did not fall in line with his desired graph. If he had chosen these six other countries [on the left side], or even more strikingly, these six countries [on the bottom right] he could have shown that increasing the percent of calories from fat in the diet reduces the number of deaths from coronary heart disease.
22 Countries with Such Data including four other groups of people
If Keys had included all 22 countries in his study, the result would have been a clutter of dots like this.
The Hunter-Gatherer Diet
Reasons Why Saturated Fats Are Good For Us
The Biologic Importance of Saturated Fat
There is good reason why 54 percent of the fat in mother’s milk is saturated fat. Cell membranes need saturated fatty acids to function properly and be "waterproof." The heart prefers saturated long-chain 16-carbon palmitic and 18-C stearic acid (over carbohydrates) for energy. Bones need them to assimilate calcium effectively. They protect the liver from the adverse effects of alcohol and medications like Tylenol. Lung surfactant is composed entirely of saturated 16-C palmitic acid, and when present in sufficient amounts prevents asthma and other breathing disorders. Saturated fats function as signaling messengers for hormone production.
Cracks in the Wall of Diet-Cholesterol Heart Orthodoxy
The American Journal of Clinical Nutrition is a leading establishment medical journal that defends the lipid hypothesis. Even this journal has backed down and is now reporting cracks in the wall of diet-cholesterol-heart orthodoxy. A meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease does not support the notion that saturated fats increase the risk of coronary heart disease, stroke, or peripheral vascular disease.
And this journal also recently published a prospective cohort study of 53,000 women and men comparing their intake of carbohydrates and saturated fats and found that replacement of saturated fats with high glycemic index carbohydrates significantly increases the risk of heart attacks.
If not cholesterol, then what causes heart disease?
Atherosclerosis is an inflammatory process brought on by eating too many carbohydrates and omega-6 vegetable oils. Stress plays a role and possibly also bacterial infection.
A deficiency of various vitamins shown here may also play a role in causing atherosclerotic heart disease, as may an excess or deficiency of various minerals.









 Cth: last makan malam pukul 8.00 malam dan keesokan harinya
anda ‘skip’ breakfast dan makan tengahari pukul 12.00 tengahari.
Cth: last makan malam pukul 8.00 malam dan keesokan harinya
anda ‘skip’ breakfast dan makan tengahari pukul 12.00 tengahari.  Maksudnya ‘puasa separuh hari’ dan
anda hanya makan 2 kali sehari (lunch, dinner)
Maksudnya ‘puasa separuh hari’ dan
anda hanya makan 2 kali sehari (lunch, dinner)